
|
LISTEN TO THIS THE AFRICANA VOICE ARTICLE NOW
Getting your Trinity Audio player ready...
|
Kenya did not find out from its president. There was no press conference, no parliamentary debate, no government health advisory. Journalists broke the news on May 27. A quarantine facility for Americans exposed to Ebola already stood on a Kenyan military air base, and it was set to open within days.
What erupted next was not a policy disagreement. It was a reckoning.
For decades, a sentence has sat at the heart of U.S.-Africa health diplomacy, rarely spoken aloud but always present in the architecture of the relationship. Your territory is available to us in ways ours is never available to you. Kenya made that sentence visible this week.
The Trump administration chose to send Americans exposed to Ebola in the Democratic Republic of Congo to Kenya rather than bring them home. The Departments of Defense, State, and Health and Human Services built the facility jointly on a Kenyan air base. American personnel staffed it. American patients would use it. Kenyan doctors had no role. Kenya’s government exercised no oversight. Nobody made a public announcement.
Washington Chose Kenya Over Its Own Backyard
The answer Kenya gave back came from doctors, lawyers, judges, and ordinary people on the street. Africa has absorbed this kind of ask quietly for generations. Why should the risk be that powerful countries refuse to carry out their responsibilities at home in African nations without complaint?
Notably, even inside the U.S. government, CDC officials pushed back hard. Agency experts warned the plan would damage recruitment for Ebola response work. Washington overruled them anyway. It did not overrule them to protect Kenyan lives. It overruled them to protect American soil.
That is the real story. Not the court order. Not the $13.5 million. Not the phone call between Secretary of State Marco Rubio and President William Ruto. Rather, this episode reveals who gets protected, who gets used, and which governments have the standing to say no.
The Outbreak Driving the Decision
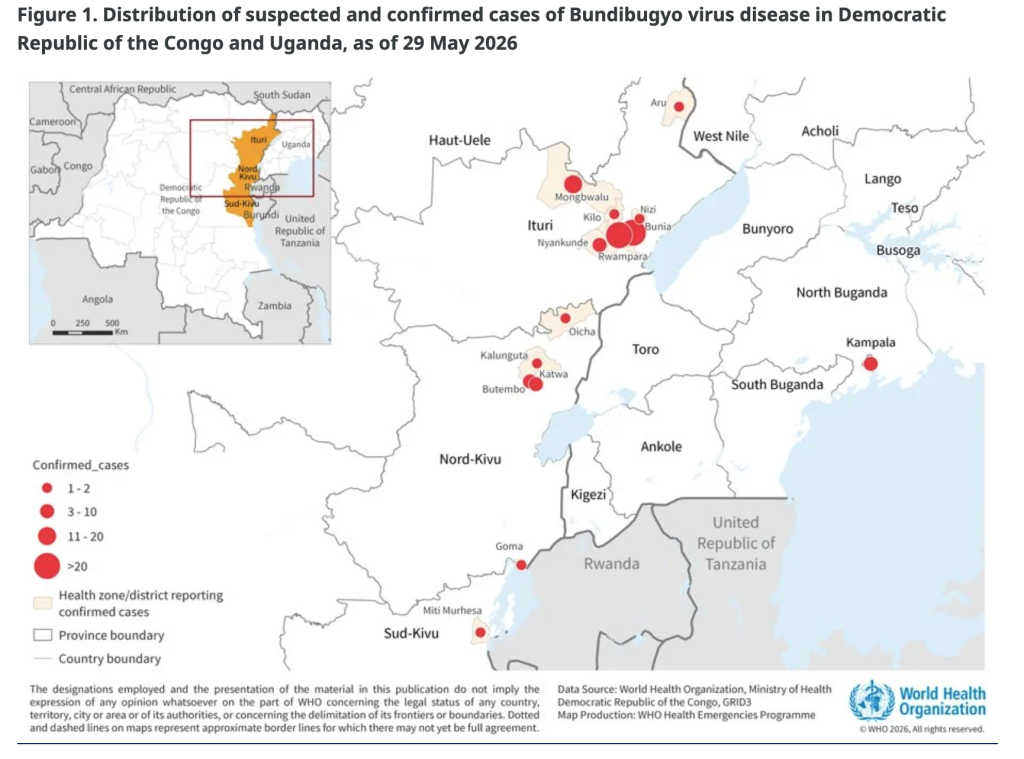
On May 15, the DRC declared its 17th Ebola outbreak. The Bundibugyo strain drives it, a rarer variant with no approved vaccine or targeted treatment. On May 17, the World Health Organization declared a public health emergency of international concern and rated the regional risk as “very high.” By May 29, more than 1,000 suspected and confirmed cases and at least 241 deaths had accumulated across the DRC and Uganda. Health experts warn that the true numbers are significantly higher, given late detection and the near-impossibility of contact tracing in a war zone.
The trigger for Washington’s urgency was specific. The Christian missionary organization Serge identified Dr. Peter Stafford, an American doctor working in the DRC, as the first confirmed U.S. case. Germany’s Charite University Hospital in Berlin received Stafford and his wife and four children for treatment and isolation. A second missionary, Dr. Patrick LaRochelle, went to the Czech Republic after exposure. Neither came home to the United States. So even before Kenya entered the picture, Washington had already established a pattern: sick Americans go to Europe, not home.
Meanwhile, WHO Director-General Tedros Adhanom Ghebreyesus landed in Kinshasa on Thursday. He warned that the outbreak in Ituri Province was “outpacing the response” and called the situation a “catastrophic collision of disease and conflict.” He appealed to the warring parties to declare even a temporary ceasefire so health workers can operate.
A Military Town That Became Ground Zero
Nanyuki sits in the foothills of the majestic Mount Kenya, in Laikipia County in central Kenya. Kenya’s Air Force operates Laikipia Air Base there. British Army training installations sit nearby. Tourism drives the local economy, drawing visitors to Mount Kenya National Park, conservancies, and some of East Africa’s finest wildlife country. Nanyuki is simultaneously one of the most militarized and most visited towns in Kenya.
Nobody told its residents what was coming.
“We have started seeing planes heading in that direction, and it looks like the quarantine area has already been set up,” Nick Karari, a Nanyuki resident, told Citizen Digital. “We are very angry because Ebola has no vaccine, no medicine, and it is our own government that decided to do this.” Joseph Muriira, a local businessman, said the facility had already hurt trade. “Hotels are closing. We are asking everyone in Nanyuki and Laikipia to come out on Monday morning without fear, because we will demonstrate to say we do not want this quarantine,” he said.
Those demonstrations are set for Madaraka Day, June 2, Kenya’s national holiday marking self-governance. The symbolism carries its own weight. Beyond the health fears, residents warned that Laikipia’s reputation as a safe, premium destination would suffer lasting damage from a decision made by Nairobi and Washington without consulting the people who live there.
The Deal Kenya’s Public Never Approved
At a White House cabinet meeting on May 27, Rubio laid out the administration’s logic plainly. “The number one priority of our foreign policy is to protect the American people. We cannot and will not allow any cases of Ebola to enter the United States,” he said.
Yet the AP confirmed that Trump himself had argued this same position in 2014, when he was a private citizen attacking then-President Barack Obama for bringing infected Americans home. “The U.S. cannot allow Ebola infected people back,” Trump wrote then. He also proposed the alternative: “Treat them, at the highest level, over there.” That over there is now Kenya.
A senior Trump administration official confirmed Thursday that the Kenyan government had approved a 50-bed quarantine unit at Laikipia Air Base. Even so, Kenya’s government made no public statement explaining the decision. Health Minister Aden Duale confirmed only that officials were in discussions with the U.S. about “preparedness and response mechanisms for Ebola,” adding that any arrangements “will be guided by Kenya’s national laws, public health regulations, biosafety and biosecurity standards.” He said nothing directly about the quarantine facility, gave no explanation for why Kenya had been chosen, and did not acknowledge that written approval already existed.
Prime Cabinet Secretary Musalia Mudavadi further defended the arrangement, arguing that Kenya was positioning itself as “a significant player within the international arena” and building approximately 16 similar intervention centers. “Surely we cannot be so stupid to go and just say we are bringing a disease and sprinkling it amongst our people,” Mudavadi said.
Kenyans remained unpersuaded. The government’s explanation arrived after the facility was already built, after courts had already intervened, and after the public had already learned the news from journalists. “It seems like the government has received substantial funding from the U.S., and it feels like they are selling us out,” Wycliff Otieno, a student in Nairobi, told reporters.
Doctors, Lawyers, and the Courts Move Fast
Kenya’s institutional response was swift and coordinated.
The Kenya Medical Practitioners, Pharmacists and Dentists Union, representing more than 10,000 doctors across public and private hospitals, issued a 48-hour strike notice and demanded full public disclosure of the deal’s terms. KMPDU Secretary-General Dr. Davji Bhimji Atellah questioned why anyone selected Kenya, more than 1,500 miles from the outbreak’s epicenter, and noted the facility made no provision for Kenyan patients despite the country’s chronically underfunded health system. His sharpest line became the week’s defining phrase.
“We will not sit back and watch Kenya be treated as a containment colony for a lethal pathogen that we did not generate. If it is too dangerous for America, it is too dangerous for Kenya,” Atellah told CNN.
The Law Society of Kenya filed a constitutional petition to nullify any agreements between the two governments, arguing Kenya lacked the necessary biosafety infrastructure. Separately, the Katiba Institute filed an emergency petition sworn by Executive Director Nora Mbagathi. It argued Kenya had become “an alternative containment site” without parliamentary oversight, environmental assessment, or public disclosure. The petition noted that Ebola management requires a Biosafety Level 4 facility, the highest category of laboratory safety, while Kenya’s facilities reach only Level 3.
Justice Patricia M. Nyaundi of the Milimani High Court acted hours before the facility was due to open on May 28. She barred the Kenyan government from establishing, operating, or facilitating any Ebola-related facility under the disputed arrangement. The next hearing falls on June 2.
“In Whose Interest Are You Acting?”
Martha Karua, former Minister for Justice and People’s Liberation Party presidential aspirant, issued a formal statement on May 30, accusing the Kenya Kwanza administration of prioritizing international interests over Kenyan welfare. “Their policy is to protect Americans first. How dare they entertain the idea that they can bring Ebola-affected people to Kenya, to protect America, but endanger the Kenyan people?” she said. Her sharpest question went directly to Health CS Aden Duale. “In whose interest are you acting, Bwana CS? Is it for wenye nchi?”
Meanwhile, talk of an impeachment motion against Ruto circulated among opposition voices as of publication, though no formal motion had been filed. Even without one, the episode had already documented a clear pattern: a president who approved a sensitive foreign arrangement in secret, told his people nothing, and left his officials to defend a deal they could not explain.
Even Washington Was Divided
The dissent, notably, was not confined to Nairobi.
CNN reported that CDC officials strongly recommended against the Kenya plan. The agency’s acting director, Dr. Jay Bhattacharya, reportedly raised similar concerns. Some officers, a CDC source told CNN, were “furious,” believing the arrangement would make recruiting and staffing for Ebola response work significantly harder.
American medical experts proved equally direct. Dr. Craig Spencer, a public health professor at Brown University who survived Ebola in 2014, told the AP he did not expect the Kenya facility to match the quality of care available in dedicated U.S. centers. Refusing to bring American Ebola patients home, Spencer said, amounted to “a moral abdication of what this country owes its own.”
After the 2014 West Africa outbreak, the U.S. government built a national network of specialized biocontainment facilities to protect American health workers abroad. It chose not to use them now.
A Warning the Continent Cannot Ignore
Sandra Babu-Boateng, host of PanaGenius and one of the sharpest analysts covering U.S.-Africa relations on the continent, had spent weeks tracking what she described as Trump’s “America First” bilateral health deals. Her breakdown of the Kenya episode cut to the core of what the money actually meant.
“America cut its own health funding to Kenya, came back, offered a smaller package, attached a biocontainment facility for American citizens to it, and called it partnership,” Babu-Boateng said. Indeed, under the bilateral health agreement Kenya signed in December, the country faces a 21% reduction in U.S. global health aid over five years. The new deal commits $1.6 billion between 2026 and 2030, a reduction of roughly $423 million compared to previous funding levels, according to KFF, a nonprofit health policy research organization.
Furthermore, Babu-Boateng warned that 22 African countries had already signed versions of these agreements, and that Kenya was not an isolated case but part of a pattern accelerating in real time. “These deals are done in secret, signed in secret, announced, if they are announced at all, in the language of partnership and generosity,” she said. “By the time the public finds out, the ink is already dry.”
Zambia, Zimbabwe, and Ghana had already rejected similar arrangements on sovereignty grounds. Kenya, however, gave written approval without a press conference, a parliamentary debate, or a public statement of any kind.
Law Society President Charles Kanjama captured the contradiction cleanly. “If America, a first-world country, is apprehensive about the health and safety of their citizens, we’re asking the Kenyan government to have the same standard,” he told CNN. “Keeping America safe while leaving Kenyans at risk of infection is a double standard.”
The Ebola outbreak in the DRC shows no sign of slowing. Diplomatic pressure on Nairobi continues to build. Washington still needs somewhere to send Americans who may be at risk of exposure. And in Nanyuki, in the foothills of Mount Kenya, on a holiday meant to celebrate self-governance, young people are planning to march.
Sovereignty, it turns out, is not a line item you negotiate away in a phone call.
(Sources: AP, May 27, 2026; CNN, May 28-29, 2026; Citizen Digital, May 30, 2026; Martha Karua Executive Office press release, May 30, 2026; WHO Disease Outbreak News, May 21, 2026; KFF Tracker, April 2026; Katiba Institute v. Attorney General, Milimani High Court, May 28, 2026; Al Jazeera, May 29, 2026; PanaGenius/Sandra Babu-Boateng, May 2026.)










LEAVE A COMMENT
You must be logged in to post a comment.